
.
Obstructive defecation, is a condition where despite straining the rectum is unable to empty its contents.
Causes
Obstructive Defecation can be due to a number of causes some of which include:
- Rectocele, where the rectum balloons outwards due to weakened walls;
- Enterocele, where loops of small bowel fall into the space between the vagina and rectum leading to bulging into these structures;
- Pelvic floor descent, where the weakened pelvic floor descends further than it should with straining;
- Rectal prolapse where the walls of the rectum collapse inwards (partial thickness) or collapse and fall out external to the anus (full thickness).
Frequently more than one condition occurs at the same time, and in rare cases all four conditions can be present.
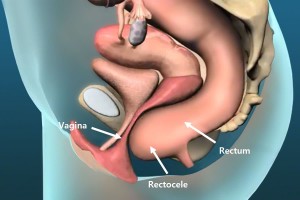
Rectocele
A rectocele results when the rectum bulges outwards on straining (figure 1). It is more common in women, and typically the bulge is at the front (anteriorly) into the vagina. It can result in the urge to apply pressure to the back (posterior) vaginal wall to facilitate evacuation.
Enterocele
Enterocele is where small bowel prolapses between the vagina and rectum causing bulging into and compression of the rectum (figure 2). It can also bulge into the vagina. If severe, the symptoms can be vomiting and abdominal distension due to small bowel obstruction.
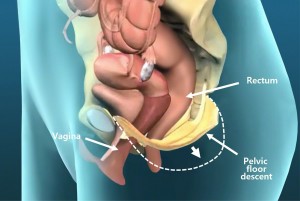
Pelvic floor descent
Pelvic floor descent is where on straining the weakened pelvic floor descends lower than it should (figure 3). This lack of fixation of the pelvis means that adequate intra-abdominal pressures cannot be obtained with straining sufficient to compress and empty the rectum.
Rectal prolapse
Rectal prolapse can be partial thickness and internal, where the lining (mucosa) of the rectum is mobile and falls into the lumen of the rectum obstructing flow, or can be full thickness and external with visible protrusion of rectum and mucosa through the anus. This often results in perianal moisture, bleeding, and some incontinence.
Symptoms
The main symptom of all of these conditions is a feeling of incomplete evacuation of the rectum on straining. Frequently, this leads to the feeling that one needs to evacuate again soon after the last attempt. This feeling can at times be so overwhelming, that a compulsion to digitally self-evacuate the rectum occurs. Full thickness rectal prolapse is often associated with perianal moisture, bleedings and incontinence.
Diagnosis
The diagnosis is often suspected based on clinical history and examination. Defecating proctography can be very useful for documenting and determining the exact cause and severity of obstructive defecation.
Ventral rectopexy
Ventral rectopexy is a procedure where a piece of bio-dissolvable mesh is used to anchor the pelvic floor and anterior wall of the rectum to the bony sacral promontory of the pelvic brim (see figure 3). This procedure is often required for patients with confirmed obstructive defecation due to partial or full thickness rectal prolapse, rectocele, enterocele and/or pelvic floor descent.
Robotic ventral rectopexy
Robotic ventral rectopexy (RVR) with the daVinci platform is gaining increasing popularity for the management of disorders that cause obstructive defecation, due to the increased ease with which suturing is able to be performed using the robot within the narrow confines of the bony pelvis. This is largely due to the ability of the articulating miniature robotic arms to perform complex fine-motor movements within a confined space.
.
Robotic Ventral Mesh Rectopexy is a procedure involving the suspension and fixation of the front of the rectum and pelvic floor to the bony sacral promontory with a bio-dissolvable mesh. In this technique, the nerves to the rectum that enter from the back and side are preserved with mobilisation only from the front of the rectum. The preservation of these nerves is thought to improve rectal function and emptying, and reduce the risk of hind gut neuropathy and resultant constipation. Preservation of these nerves also prevents disorders of sexual function and fertility. There is no evidence that recurrence rates are higher with bio-dissolvable mesh compared with permanent mesh. The bio-dissolvable mesh also avoids the long-term complications of mesh infection and erosion reported with permanent mesh.
Robotic versus Laparoscopic Surgery
Robotic ventral mesh rectopexy with the da Vinci® platform is gaining increasing popularity and beginning to replace laparoscopic surgery due to the increased ease with which suturing is able to be performed using the robot within the narrow confines of the bony pelvis. This is largely due to the ability of the articulating miniature robotic arms to perform complex fine-motor movements within a confined space. The extra third arm also allows for excellent retraction within the narrow pelvis, and the three dimensional magnified view allows for visualization and preservation of the pre-sacral nerves preventing hind gut, sexual and fertility dysfunction.

The latest Xi da Vinci® robot, has narrow instruments and a camera less than 8mm in width, allowing all ports to be less than 8mm in size. This has the advantage of smaller cuts and less pain and early discharge and return to normal activities. The ability of the camera to fit through any of the 8mm ports (a features not present with earlier da Vinci® models) also allows for greater freedom and interchange of instruments when required, making multi-quadrant surgery much easier.
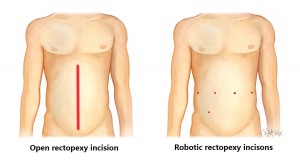
The 8mm incisions with the xi da Vinci® model are usually five in number as shown above, with one for the camera, three for robotic instruments, and one for the surgical assistant to assist with the passing of sutures, equipment as required.
Complications after ventral rectopexy
Complications after ventral rectopexy are uncommon. The risk of constipation is reduced by this procedure which involves only anterior (i.e. ventral) dissection and avoids posterior rectal mobilisation, and therefore avoids damage to the posterior autonomic nerve supply to the rectum. Recurrence rates are less than 5%[1], being much lower than perineal procedures where recurrence rates are as high as 20-30%[1]. Mesh erosion into the vaginal has been reported, and this risk is significantly reduced by using a dissolvable mesh such as Surgigis®, which is an 8 ply mesh that is made from porcine submucosal collagen[1]. There is no evidence that using a dissolvable mesh increases recurrence rates [2]. Dissolvable sutures such as PDS also reduce the risk of long-term infection, but do increase the risk slightly of recurrence. Intervertebral disk infection has been described as a rare complication occurring in 0.3% of cases from fixation of the mesh to the bony sacral promontory with 2 cases reported in a review of over 728 cases [2]
What to expect prior to surgery for rectal prolapse
Clear Fluids
You will need to have only clear fluids the day before your surgery. Clear liquids are those that one can see through. When a clear liquid is in a container such as a bowl or glass, the container is visible through the substance. Examples of clear fluids include water, broth, apple juice, jelly, sports drinks such as Gatorade®, Lucozade® and Gastrolyte®. Try to drink at least 3-4 litres the day prior to your surgery.
Bowel Preparation
You will also require bowel prep to clean your colon. Take a Pico-sulfate (Picolax®) sachet (mixed in a glass of water) at 2pm, 4pm and 6pm the day before your procedure. If you are prone to constipation, the 4pm Picolax is replaced with a sachet of Glycoprep (mixed to a litre with water). You can purchase these from your chemist without needing a prescription.
Nil By Mouth
You need to be nil by mouth (i.e. no liquids) from midnight the night before if your surgery is scheduled for the morning, or from 6am if scheduled for the afternoon.
Admission Time
The exact time for your admission is finalised the day prior and you will receive a phone call in the morning at about 10am to inform you what time to present. This is normally 2 hours prior to the planned start time.
What to expect after surgery for rectal prolapse
Diet
Immediately after your procedure you will be commenced on free fluids (semi thickened fluids such as custard, yoghurt, thin porridge). Once you have passed flatus, and any nausea has settled you will be commenced on a light diet.
Pain Relief
You will be given a Patient Controlled Analgesia (PCA) device to administer your own pain relief for the first 24 hours, then this will be replaced with oral pain killers (usually paracetamol, and a nonsteroidal such as Celcoxib® or Nurofen®, and if needed oral oxycodone (oxycontin®).
Laxatives
You will be on regular laxatives (Movicol®) from day 1, and should remain on this for 6 weeks. The dosage is individualised, with huge variation between patients. The usual starting dose is one Movicol® twice daily. This can be halved or doubled or quadrupled depending on the response. The aim is soft stool to avoid straining.
Exercise
Walking is encouraged from day one, as this improves your recovery and prevents against developing a venous clot and pneumonia. Gentle swimming or cross-trainer or cycling can occur after 48 hours. No vigorous running, jumping or exercises are recommended for 6 weeks after surgery.
Dressings
Water proof Comfeel® dressings will cover each of your 8mm incisions, and can be removed 7 days after surgery and simply left open.
Discharge Home
You will be discharged from hospital once you have opened your bowels and are tolerating a normal diet. This can range from 3 days to a week.
Regular medications
If not already done so, you are to go back on all your regular medications on discharge.
Follow-Up
Please ring 1300 265 666 to organise a follow-up appointment with your surgeon at 2-6 weeks after your procedure.
References
- Samaranayake CB, Luo C, Plank AW, Merrie AE, Plank LD, Bissett IP. Systematic review on ventral rectopexy for rectal prolapse and intussusception. Colorectal Dis. 2010;12:504–12.
- Smart NJ1, Pathak S, Boorman P, Daniels IR. Synthetic or biological mesh use in laparoscopic ventral mesh rectopexy–a systematic review. Colorectal Dis. 2013 Jun;15(6):650-4.